
This Evidence Paper examines the role of migration and the impacts of immigration policy on the UK’s health and care workforce. It is part of a series of briefings by the Migration Observatory with ReWAGE.
-
Key Points
- The health and care industries faced significant staff shortages in 2023, with high vacancy rates in the NHS in England despite a growing clinical workforce.
More… - The UK immigration system admitted unprecedented numbers of overseas health and care workers in the year ending March 2023: almost 100,000 people, making up the majority of Skilled Worker entry visas.
More… - The NHS in England has become more reliant on overseas health professionals over the past five years. Half of secondary-care doctors registered with the General Medical Council in England in 2022 had received their primary medical qualification abroad (excluding trainees).
More… - Overseas health and care workers come primarily from non-EU countries. EU nurses played a substantial role in NHS recruitment in the early 2010s, but this was a temporary phenomenon.
More… - Reliance on international recruitment varies across the nations and regions of the UK and among NHS hospital trusts.
More… - Immigration policy has not been a barrier to the large-scale recruitment of overseas health professionals post-pandemic. Increased reliance on overseas health and care workers brings financial benefits but also creates risks to sustainable recruitment in the future, as well as risks of exploitation in the care workforce.
More…
- The health and care industries faced significant staff shortages in 2023, with high vacancy rates in the NHS in England despite a growing clinical workforce.
-
Understanding the Policy
... Click to read more.Immigration rules for health and care workers
Non-UK health professionals can come to the UK to work in the NHS or private sector health and care roles through various routes. Most health and care jobs are eligible for long-term skilled work visas, and licensed employers can sponsor non-UK citizens to come to the UK for work as long as they are willing to pay the fees and meet salary requirements.
Required salaries are set using NHS pay scales. Care workers, who are not covered by NHS pay scales, must receive at least £20,960 as of April 2023. Health and care workers sponsored to work in the UK receive a Health and Care Visa, which is effectively the same as a Skilled Worker visa but with lower fees and fast-tracked visa processing. This visa also covers trainees who have completed medical school and have moved into clinical training positions. After five years of work (whether as a trainee or a fully qualified professional), visa holders can apply for permanent status or settlement if they still work in an eligible role. Care workers became newly eligible for work visas under the post-Brexit immigration system – senior care workers in December 2020 and care workers in February 2022.
Not all migrants working in health and care are on work visas sponsored by their employers. Many already have permission to be in the UK in other immigration categories, e.g. as family members or refugees. Before the end of free movement and the introduction of the post-Brexit immigration system, EU, EEA and Swiss workers and their family members could come to the UK for health and care jobs without a visa. Asylum seekers waiting for a decision on their applications usually cannot work, but once they have waited for at least a year, they can apply for the right to work in shortage occupations.
International recruitment
International recruitment is a formal part of NHS workforce plans for each of the devolved administrations. NHS trusts and boards (i.e. legal organisations within the NHS that run services such as hospitals) can receive financial support to facilitate international recruitment and may conduct recruitment campaigns overseas. NHS employers are expected to follow the World Health Organisation’s Code of Practice for ethical international recruitment. The Code says that health employers should not conduct active recruitment from listed countries experiencing severe health workforce problems. However, NHS employers can still recruit residents of these countries if the workers apply independently, e.g. after identifying vacancies on the NHS Jobs website. Some analysts have raised questions about compliance with the Code. Some countries that would otherwise be ‘red listed’ have memoranda of understanding (MoUs) that allow international recruitment under agreed conditions.
People who received their primary medical qualifications abroad need to have their qualifications recognised in the UK. For doctors and nurses, recognition typically involves English language and practical assessments. When the UK was an EU member state, nurses, midwives, doctors, dentists and pharmacists had their EU qualifications recognised automatically. After Brexit, transitional arrangements continue to allow ‘near-automatic’ recognition of the same EU qualifications. This system is due to be reviewed in 2023.
-
Understanding the Evidence
Data on the health and care workforce have uneven geographical coverage. Some data cover all nations while other data only cover England. ... Click to read more.This Evidence Paper uses NHS Digital data on the Hospital and Community Health Services (HCHS) workforce in England. This data source provides relatively high-quality data on the NHS workforce by role and location within England. However, an important caveat with this dataset is that the recording of nationality has improved over time, reducing the share of workers whose nationality is recorded as unknown. This change means that the figures will likely overstate the absolute increase in each known nationality group. It can thus be more helpful to examine changes over time by looking at percentages of those staff with known nationality. Unless otherwise specified, percentages of the NHS in England staff by nationality exclude those with unknown nationality. Scotland, Wales and Northern Ireland do not publish comparable data on the NHS workforce. Note that the HCHS data exclude primary care (i.e., GPs) and non-NHS provision – including most care work, which is commissioned by local authorities.
The NHS in England HCHS data groups nationalities into three categories: UK and Irish, EU excluding Irish, and non-EU. For simplicity, this Evidence Paper uses the terms ‘EU’, ‘non-UK’ and ‘overseas’ workers, not including Irish citizens. The data come from the NHS HR and payroll system, the Electronic Staff Record (ESR). Within ESR, the nationality is self-reported by the individual staff member. It is recorded when an individual is first appointed and can also be changed by the individual at any time in the course of their employment, for example, if they become a UK citizen—although it is not clear how common it is for staff to do this in practice. As a result, there is some uncertainty about the extent to which the figures represent current vs. original nationality.
The NHS also publishes vacancies data. These do not necessarily represent unfilled roles; the Nuffield Trust estimates that most vacancies are filled temporarily (e.g. using locums) while longer-term recruitment takes place (Nuffield Trust, 2022). These vacancies are for jobs that NHS employers have the budget to recruit and do not necessarily reflect an optimal number of people to be recruited.
This Evidence Paper also uses UK-wide data on the number of doctors on the General Medical Council (GMC) register. These figures cover the whole of the UK and include a variable for the doctor’s location, although some doctors do not have a location recorded.
The health and care sector faced significant staff shortages in 2023
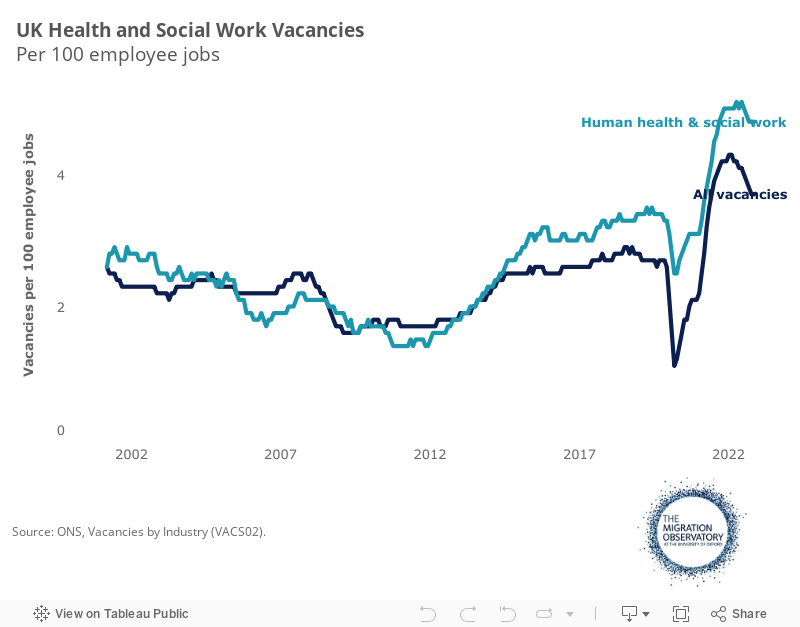
The health and care sector is currently facing significant pressures on its workforce, in what the House of Commons Health and Social Care Committee (HSCC) has described as a “workforce crisis”. As in several other industries, vacancy rates in health and care have increased sharply since the pandemic (Figure 1). The Office for National Statistics (ONS) estimated that vacancies in the UK’s health and social work sector peaked at 217,000 in July to September 2022 before falling somewhat in late 2022 and early 2023. (Note that these figures include social work jobs that are not part of the health and care sector.) At its peak, the vacancy number was equivalent to five vacancies per 100 employee jobs.
Figure 1a
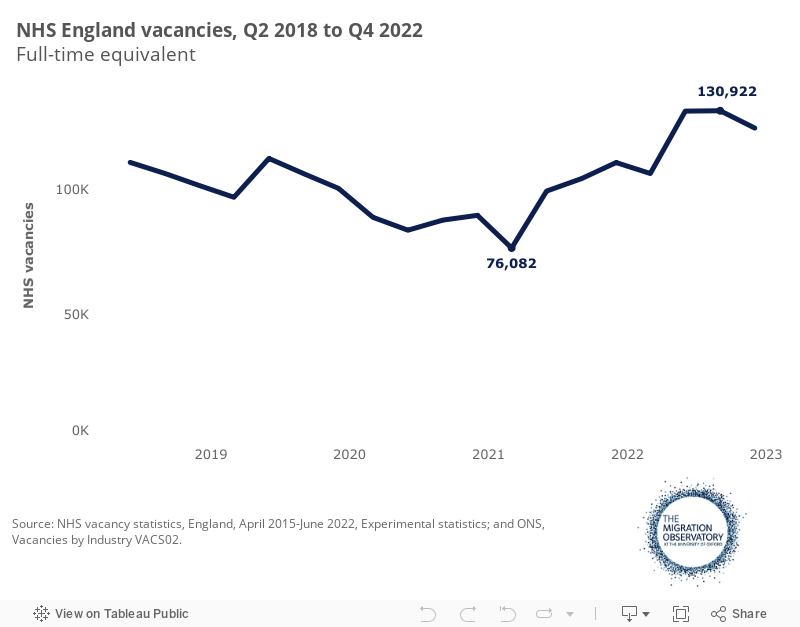
The NHS alone was advertising 124,000 full-time equivalent jobs in England in the last quarter of 2022, indicating a vacancy rate of 8.9%. Note that NHS vacancies are usually filled temporarily (e.g., using agency staff and at a higher cost), so these figures do not represent entirely unfilled posts.
Figure 1b
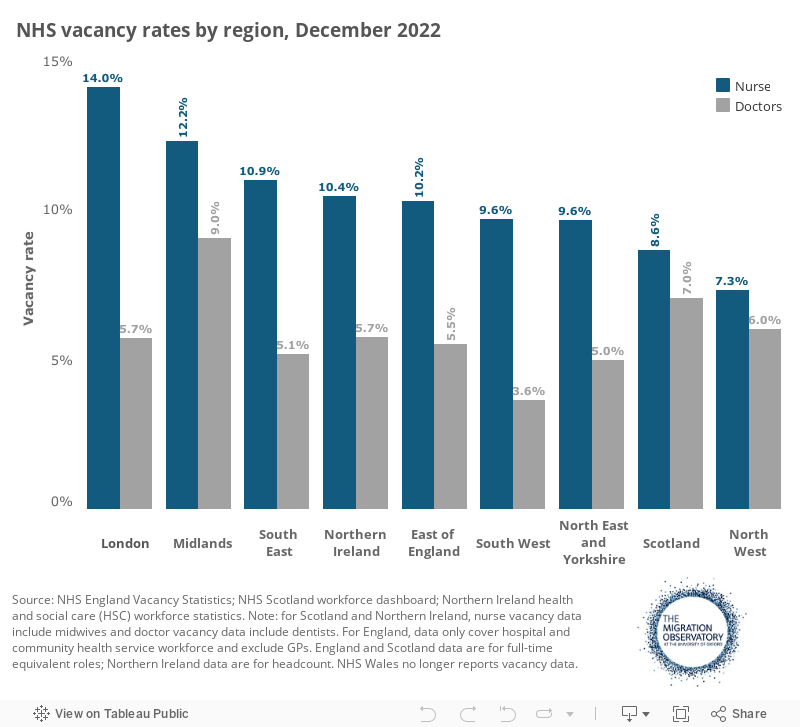
NHS vacancy rates in England were higher for nurses (10.8% in Q4 2022) than for doctors (5.9%). Vacancy rates also varied by region. Nursing vacancies were highest in London (14%), where the vacancy rate for mental health nurses exceeded 20% (Figure 2). The high cost of living in London (particularly housing and transport) has been a key factor making the capital less attractive to nurses. A Royal College of Nursing (RCN) survey in 2019, for example, found that 57% of nurses wanted to leave London within the following five years, with many citing the cost of living as the primary barrier to remaining in the capital. An Institute for Fiscal Studies (IFS) analysis shows that pay supplements in some regions do little to compensate for the higher cost of living in London and the South of England and that retention of nurses is worse in high-cost areas.
Figure 2
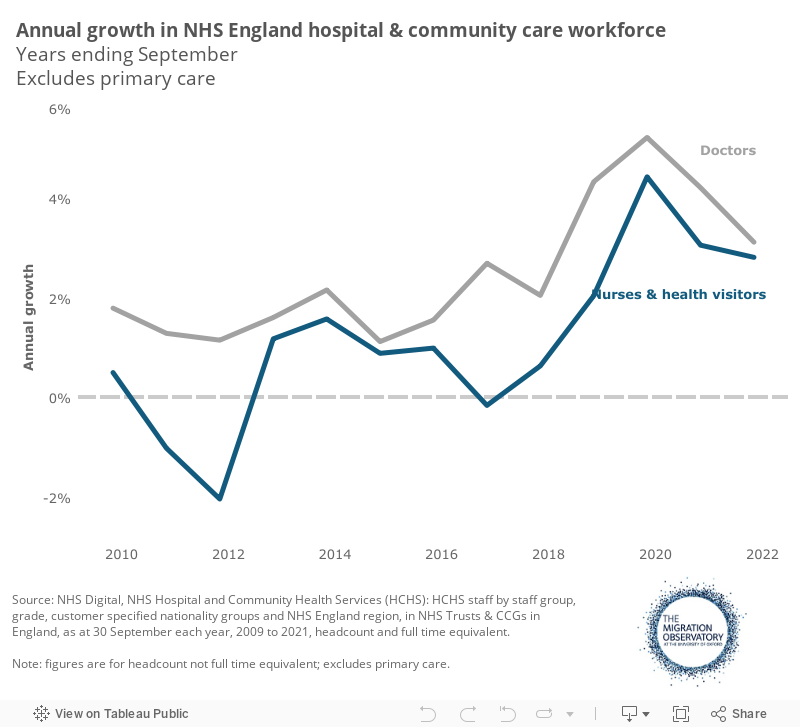
High vacancy rates have persisted despite strong growth in the size of the NHS workforce over the past few years (Appendix Figure A). For example, the NHS in England hospital and community health services saw a 22,300 (8%) increase in full-time equivalent nurses and health visitors and an 11,200 (10%) increase in doctors from September 2019 to September 2021.
At the same time, however, demand for health professionals has increased, and productivity has fallen. In the long term, demographic change and the ageing population have increased demand for health and care, while improvements in medical technologies mean that more (and more complex) health interventions are now possible, requiring the staff to deliver them. The Covid-19 pandemic has further increased demand for health services due to long-term illness and elective care backlogs, according to the Department of Health and Social Care. IFS analysis found that even despite an increase in staffing, as of 2022, the NHS was treating fewer patients across a range of areas of care (though not GP appointments, which had increased). That is, productivity had decreased for reasons that may include fewer hospital beds available for non-Covid patients, difficulties discharging patients and sicker patients.
Against this backdrop, the Health Foundation projected in July 2022 that even though the government was on track to meet its target of 50,000 additional full-time equivalent nurses by March 2024 – in large part due to international migration, as discussed below – these increases would not be sufficient to meet projected demand.
Unlike the secondary care workforce, the number of fully-qualified general practitioners (GPs) did not increase in 2020 and 2021, and in FTE terms, declined gradually from 2017 to early 2022. The Conservative Party’s 2019 manifesto pledge to increase GP numbers by 6,000 was not expected to be met as of mid-2022.
Recent analytical reports also identified severe problems recruiting staff in the care industry, primarily due to persistent underfunding, which has kept wage rates low and made it difficult to attract workers into the sector and away from competing industries.
The immigration system brought unprecedented numbers of overseas workers into the health and care workforce in 2022-3
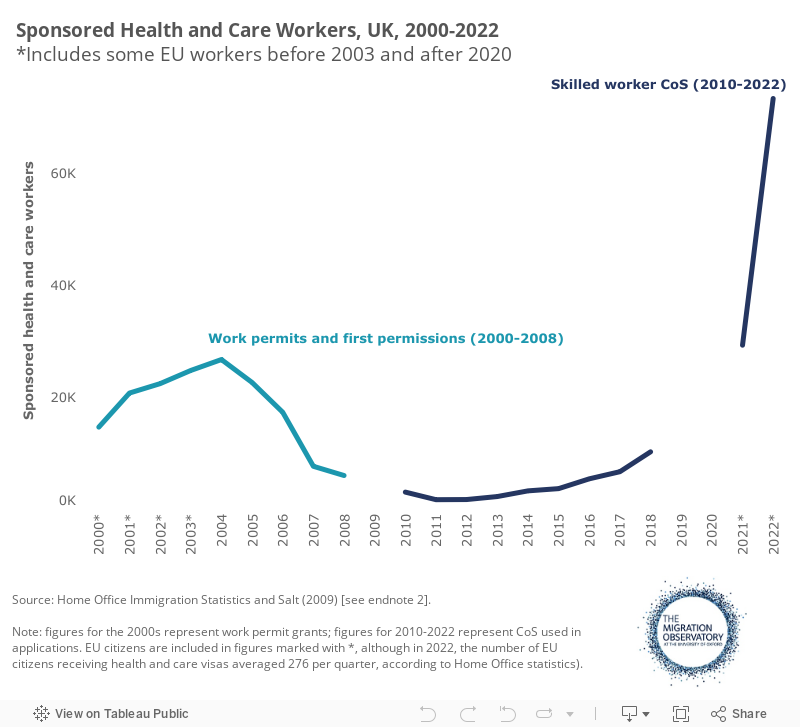
Against a backdrop of staff shortages, the recruitment of non-EU citizens on skilled work visas in the health and care sector increased from 2017 onwards, with a particularly sharp increase in 2021 and 2022 (Figure 3).
In 2022, just over 73,000 main applicants were sponsored for skilled work visas in the health and care sector (Figure 3), and the number continued to rise in early 2023 (Table 1, below). The scale of recent health workforce recruitment from overseas greatly exceeded the previous peak, which took place in the early 2000s after the Labour Government promised a substantial increase in NHS staffing. During that period, work permit grants peaked in 2004 at just under 26,600 main applicants. The increase in visas granted in recent years does not result simply from the fact that the visa statistics now include EU citizens: in 2022, the number of EU citizens receiving Health and Care visas averaged only 276 per quarter (Figure 3).
In other words, the health and care sector has never admitted such large numbers of work visa holders as in the immediate post-pandemic period under the post-Brexit immigration system. Health sector visa grants were also considerably lower during historical international recruitment periods in the 1950s to 1990s.
Figure 3
The increase in non-EU work visa holders was initially driven primarily by nurses, but this changed in 2022 with substantial recruitment in care and senior care worker roles. Senior care workers became eligible for skilled work visas in January 2021, and care workers in February 2022. In the year ending March 2023, just under 26,000 nurses and approximately 57,700 care or senior care workers received entry visas. Clinical and managerial roles in health and care comprised 59% of all entry visas issued under the skilled worker category that year (Table 1). As a result, the health and care sector has been the most important driver of overall increases in work-related migration.
Table 1
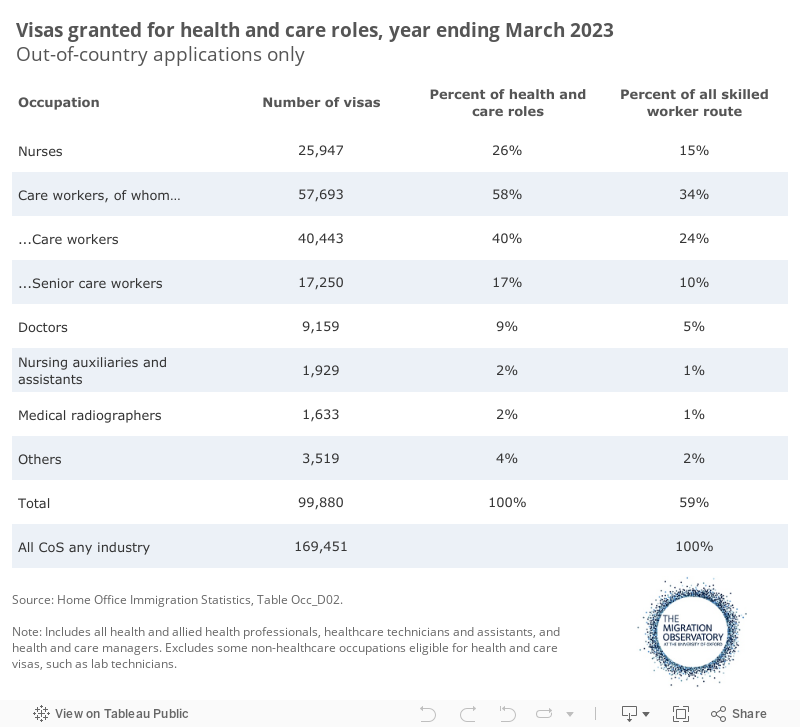
The move to make care workers eligible for skilled work visas followed a recommendation by the Migration Advisory Committee, which concluded that the end of free movement after Brexit had exacerbated existing shortages caused by poor pay and conditions in the sector. However, the number of care workers sponsored on skilled work visas in 2022 appears to have greatly exceeded the number who would have come annually under free movement. While precise figures on annual numbers of EU care workers joining the workforce under free movement are not available, Skills for Care estimates that there were only 103,000 EU national workers in the care sector in England in 2021-22. These workers would have moved to the UK over a period of many years when freedom of movement was in place. As noted above, roughly 57,700 care and senior care workers were sponsored on entry clearance work visas in the year ending March 2023 alone, primarily from non-EU countries. In other words, a number of workers equivalent to more than half the entire EU national care workforce was sponsored to come to the UK in a single year under the post-Brexit immigration system.
The share of workers in the residential care sector who worked for an employer that held a sponsor license increased from 10% to 39% from February 2022 to March 2023 – the first 13 months after care workers became eligible for skilled work visas. Skills for Care found that the share of new starter employees who had arrived in the UK from overseas to start an adult care job had increased from 2% in 2020-21 to 11% in 2022, suggesting a substantial increase in the importance of overseas recruitment in the care industry, despite the end of free movement. (Note that data for previous years are not available, and 2020-1 figures may have been unusually low due to the pandemic.)
The NHS in England has relied on a growing share of non-UK staff to increase the size of its clinical workforce
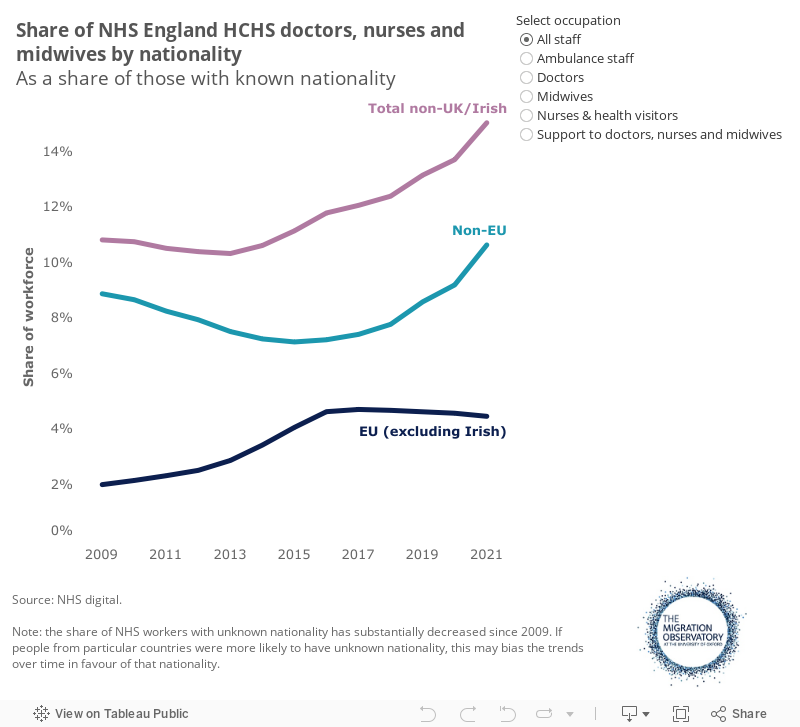
The share of overseas nationals among doctors, nurses and midwives in the NHS in England’s hospital and community health service workforce increased from a low of 15% of those with known nationality in September 2013 to 21% in September 2021. Doctors were more likely to be non-UK or Irish nationals (30%) than nurses and health visitors (21%) or midwives (6%). The pattern in Wales is different: there, the share of non-EU workers has been broadly stable while the share of EU workers has declined.
Figures on nationality may understate the role of migrants in the health workforce because they may exclude some people who migrated to the UK had then become UK citizens (see ‘Understanding the Evidence’ above). A large majority of non-EU citizens who are eligible for citizenship become UK citizens within ten years of migrating to the UK. Changes in citizenship may explain why, while 30% of doctors in the NHS in England’s hospital and community health services were non-UK or Irish citizens in September 2021, 50% of doctors on the UK General Medical Council (GMC) register in England in 2022 had received their primary qualification from abroad, excluding GPs and trainees (Figure 5, below).
Figure 4
The increase in the NHS in England’s non-UK workforce has been part of a larger expansion of the number of clinical staff. In particular, the number of doctors and nurses of all nationalities increased more from 2018 to 2021 than in previous years (Appendix Figure A). Medical and nursing training takes several years, which means that in the short term, it is difficult to sharply increase the size of the workforce using recruitment of UK nationals. Migration is thus often positioned as a short-term solution alongside longer-term ones that focus on local recruits. For example, the NHS in England Interim People Plan (2019) noted that while international recruitment would help to “increase supply rapidly,” the NHS must “drive towards a supply balance for the nursing that meets the demands of health and care services, centred on a domestically grown workforce”.
In the three years to September 2021, non-UK or Irish nationals accounted for most of the expansion in the number of doctors and nurses employed in the NHS in England’s hospital and community health services workforce. The net increase during this period was around 8,600 for UK or Irish doctors, compared to 9,700 for overseas workers (FTE figures). Among nurses, the number of UK or Irish nationals increased by 14,500, compared to 22,200 for other nationals, according to NHS Digital data.
Will the overseas recruitment boom persist?
In the past, spikes in overseas recruitment have been temporary. For example, large-scale recruitment of overseas nurses in the early 2000s abruptly declined in the middle of the decade when increasing numbers of domestically trained nurses started to enter the workforce. However, the scale of international recruitment in 2021-2 was much larger than the previous peak, as noted above, suggesting greater reliance.
The UK’s ability to ‘ramp down’ the current high levels of international recruitment and increase employment from within the UK will depend on a combination of factors, including demand, retention of existing health professionals and whether increases in training capacity domestically are sustained. For example, the number of nurses starting university nursing training in the UK increased by over 7,500 (more than a quarter) in the three years to 2021/22. This rise followed official targets to increase nurse training and clinical placements, which had been an important factor holding back the size of the UK-trained workforce in recent years. However, there was also a 7,800 increase in nurses leaving the NHS in England in the three years to June 2022. If retention difficulties persist, it will undermine attempts to boost the workforce by increasing training places.
UK healthcare employers have been able to increase overseas recruitment sharply, as the previous figures have shown. However, some organisations have recommended reducing the reliance on international recruitment due to the concern that global competition for health professionals could make this source of source of workers less reliable in future.
Overseas health professionals come primarily from non-EU countries
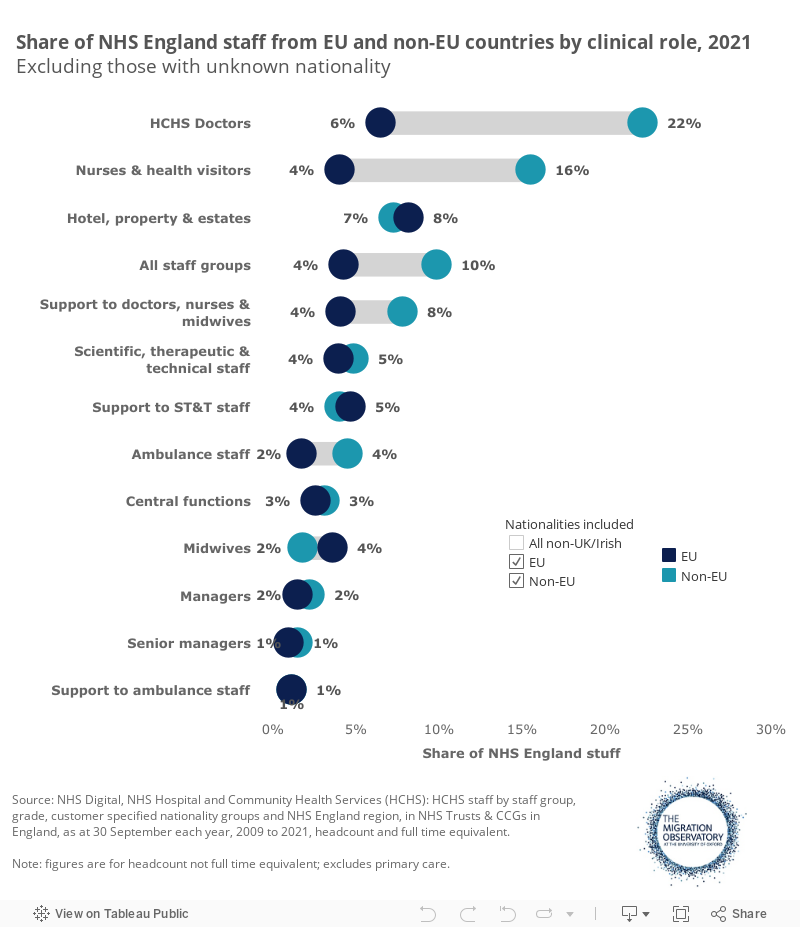
Traditionally, most non-UK or Irish staff in the NHS have been from non-EU countries rather than the EU. EU citizens joined the NHS hospital and community health workforce in England in substantial numbers during the mid-2010s, although the share of non-UK nationals from the EU nonetheless peaked at 39% in 2016 and fell back to 30% by September 2021. In September 2021, 20% of non-UK nurses and health visitors working in the NHS in England were EU citizens, as well as 22% of doctors and 34% of people in support roles to nurses, doctors and midwives (Appendix Figure B).
Doctors
Among doctors, non-EU citizens have always made up the majority of overseas NHS joiners in England. Even during the peak of EU health workforce recruitment from 2013-2016, 90% of overseas doctors were from non-EU countries. Note that this pattern does not apply in all specialities, though. Some—such as anaesthetics and cardiothoracic surgery—have been more reliant on EU workers and more affected by the end of free movement than others, according to Nuffield Trust analysis.
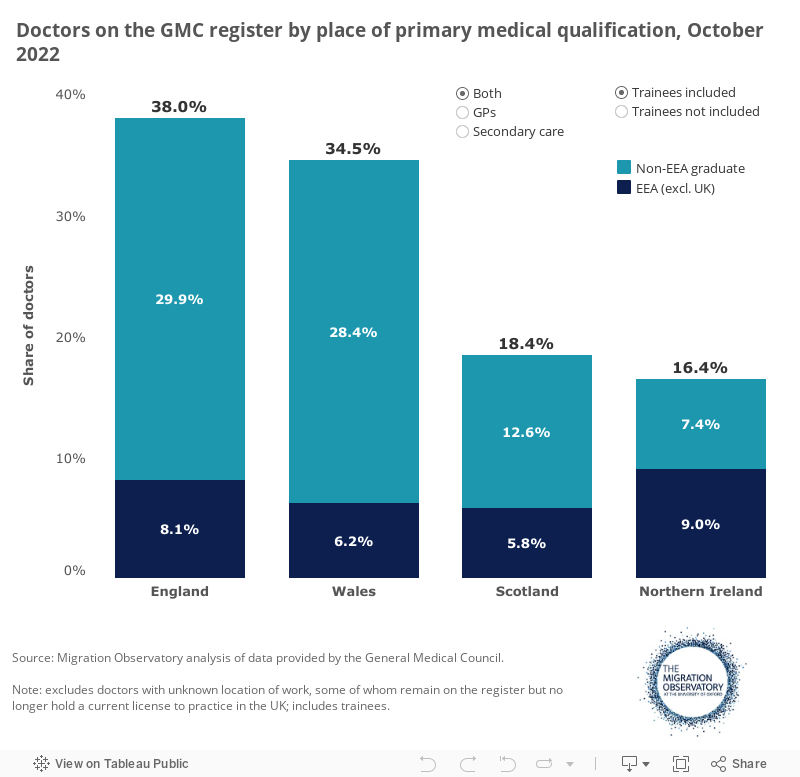
Data on doctors on the General Medical Council (GMC) register give a picture of the doctor workforce for the whole UK. Non-EEA trained doctors were the majority of overseas-trained doctors in England, Wales and Scotland in October 2022. Northern Ireland was the exception, with a majority coming from EEA countries (including Ireland). Overall, non-UK trained doctors made up 50% of the secondary care doctor workforce in England (excluding trainees) in October 2022, with substantially lower shares in Scotland and Northern Ireland (Figure 5). Across the UK as a whole, 47% of doctors with a known practice location were trained in EEA or non-EEA countries.
In 2022, the largest individual nationalities of doctors sponsored for UK skilled worker visas were India (20% of sponsored doctors), Nigeria (15%), Pakistan (12%) and Egypt (9%). See Table 2 below for further data.
Figure 5
Nurses
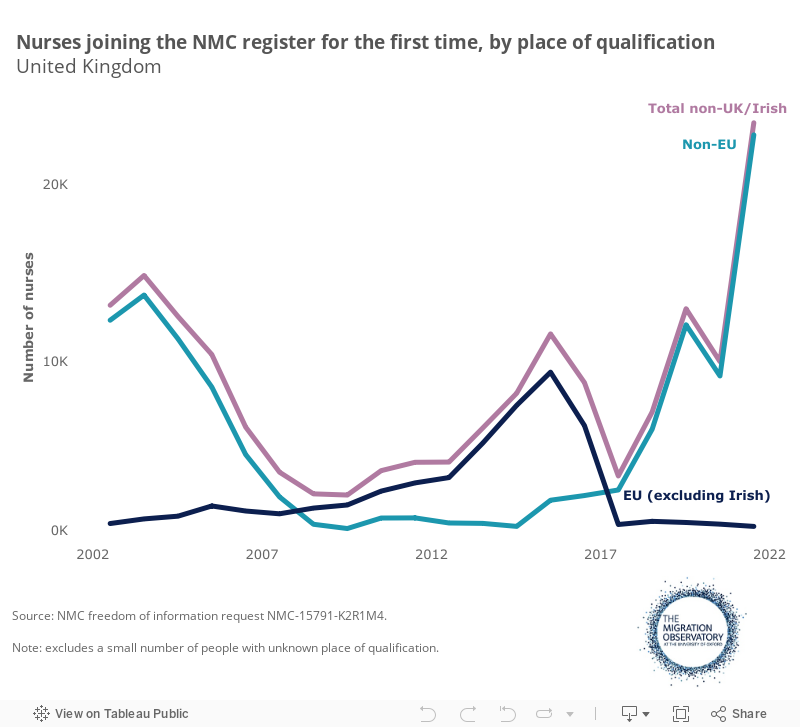
The main countries of origin for people joining the Nursing and Midwifery Council (NMC) register for the first time have shifted dramatically over the past decade (Figure 6). During the mid-2010s, people trained in EU countries were the main source of new joiners. Higher EU recruitment was a temporary phenomenon during a period in which overall EU migration to the UK was unusually high by historical standards. The number of EU nurses joining the register fell sharply after the EU referendum, however. This decline took place at the same time that overall EU migration was falling sharply as the UK became less attractive to EU migrants across the board and was also exacerbated by an early 2016 change in licensing requirements for people with EU qualifications. By 2021/2, however, 97% of overseas-trained people joining the NMC register were trained in non-EU countries.
The share of overseas-trained professionals on the Nursing and Midwifery Council register was under 21% in March 2023 across the UK as a whole, up from around 15% in March 2018.
In 2022, the largest individual nationalities of nurses sponsored for UK skilled worker visas were India (46% of sponsored nurses), the Philippines (22%), Nigeria (14%), Ghana (6%) and Zimbabwe (3%). See Table 2 below for further data.
Figure 6
Care workers
In 2022, 99% of care workers sponsored for work visas in the UK were from non-EU countries, with only 1% coming from EU countries, according to data obtained through a Freedom of Information request (75614). The top countries of citizenship for workers using Certificates of Sponsorship (CoS) in 2022 were India (33%), Zimbabwe (16%), Nigeria (15%) and the Philippines (11%).
Table 2 shows the top nationalities for doctors, nurses, and care workers in 2022. The data come from provisional management information that does not align with official visa grants statistics but nonetheless give some indication of the main countries of origin for health and care workers.
Table 2
Certificates of sponsorship (CoS) used for out-of-country visa applications, 2022
| Nationality | Code of practice status (March 2023) | Doctors | Nurses | Care workers |
|---|---|---|---|---|
| India | Green | 20% | 46% | 33% |
| Philippines | Green | 0% | 22% | 11% |
| Nigeria | Red | 15% | 14% | 15% |
| Ghana | Red | 1% | 6% | 5% |
| Zimbabwe | Red | 0% | 3% | 16% |
| Kenya | Amber | 0% | 2% | 2% |
| Nepal | Amber | 1% | 1% | 1% |
| Pakistan | Red | 12% | 1% | 3% |
| Sri Lanka | Green | 6% | 0% | 2% |
| Egypt | Green | 9% | 0% | 1% |
| Others | n/a | 36% | 6% | 12% |
Source: Migration Observatory analysis of FOI 75614; WHO Code of Practice list status is from NHS employers: https://www.nhsemployers.org/articles/code-practice-red-and-amber-list-countries. Note: Certificates of sponsorship data are from provisional management information. Some CoS used in applications will not lead to a visa grant. Nationalities shown are the top 10 countries for the combined total of doctors, nurses and care workers. Note that the Code of Practice data applies to the country of residence, whereas sponsorship data are for the country of citizenship.
Some of the top countries of origin for overseas health and care workers are ‘red-listed’ countries where NHS employers are expected not to carry out active recruitment activities. However, this does not stop individual applicants from applying proactively for jobs advertised on the NHS Jobs website.
Reliance on international recruitment varies across England
Some parts of the NHS in England rely more heavily on overseas health professionals than others. In September 2021, non-UK or Irish citizens comprised just under a quarter of London’s hospital and community health workforce but only 7% in the North-East and Yorkshire (Figure 7). Different regions’ reliance on overseas health professionals also varies by role. For example, most regions have a higher share of overseas doctors than nurses, but this is not the case in London and the South East. In London, NHS hospital and community health employers rely more heavily on overseas citizens as nurses (32%) than doctors (27%). The share of doctors in London with non-UK or Irish nationality is below the England average, which is unusual for London, where migrant shares across the workforce and population tend to be higher than in other regions.
Figure 7
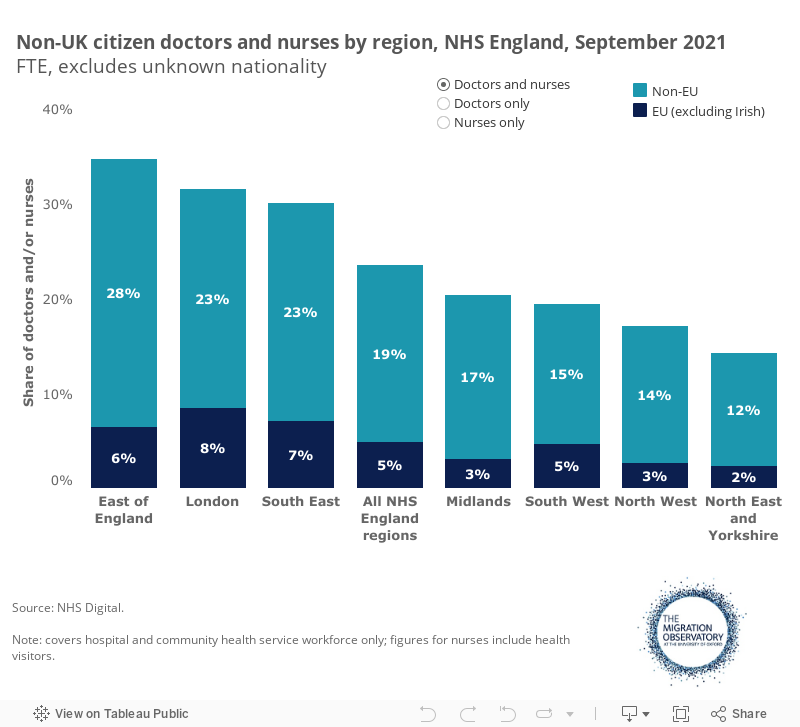
In September 2021, non-EU nationals outnumbered their EU counterparts in every region of England. Relative reliance on EU workers was greatest in London, where EU citizens made up 36% of overseas doctors and 24% of overseas nurses and health visitors. A recent study found that the existing make-up of the workforce influenced overseas nurses’ location decisions and that trusts that already employed workers of the same nationality were considered more attractive. Nursing positions outside of London were also more attractive for some nurses because of the high cost of living in the capital.
Implications for the development of policy
Heavy reliance on overseas health and care workers brings financial benefits but also creates important risks.
Shortages in the health and care workforce do not seem to result from immigration policy. The high number of health and care visas that the UK has issued in recent years suggests that the UK has been an attractive destination, and employers in the sector have typically been able to overcome the barriers that immigration policy can create.
Some health and care employers may find it more difficult to recruit non-UK workers than others. For example, the end of free movement may have had a greater impact on certain specialisms that were unusually reliant on EU citizens. The Health and Social Care Committee has also pointed out that it can be more difficult for GP practices to sponsor workers because they are small organisations, and the shorter duration of their training means they will not necessarily have permanent immigration status by the end of their GP training. Nonetheless, it is fair to say that immigration policy has not prevented a large increase in recruitment of overseas health and care workers post-pandemic.
In the medium to long term, UK health and care employers’ ability to recruit sufficient staff is likely to depend primarily on policies to improve recruitment and retention among domestically trained workers, who make up the majority of the workforce. However, the NHS produces workforce plans on an irregular basis, and the care sector has no formal workforce planning. An independent expert panel set up by Health & Social Care Committee in 2022 also criticised the lack of strategic planning for the care workforce. The Migration Advisory Committee published a report in early 2022 arguing that poor pay and conditions had led to substantial shortages in care. It recommended increasing the salary for care workers above the minimum wage to attract and retain workers in the sector. It also recommended making care workers eligible for skilled work visas. The Home Office implemented the immigration recommendation in 2022 but, at the time of writing in June 2023, no action had been taken on the pay recommendation. Poor pay and conditions will likely be an important factor behind the surprisingly high demand for care workers sponsored from non-EU countries in the past year.
The UK benefits from health and care workers whom it has not paid to train (although there may be some hidden induction costs for newly recruited international staff). However, high reliance on overseas workers—if it persists—may also create risks for the UK health and care system. First, changes in other countries’ demand for international health workers could affect NHS employers’ ability to recruit in future (for example, if a large country like the United States started to recruit more aggressively from abroad). Second, international recruitment is helpful for employers in the short run but does not necessarily address the underlying challenges in recruiting and retaining domestically trained workers, who still make up most of the workforce. In future, retention challenges may affect internationally recruited workers too, especially after they receive Indefinite Leave to Remain and can work in other jobs more easily.
Third, and particularly in the care sector, work visas can bring risks of exploitation. The Director of Labour Market Enforcement (DLME) has identified care as a high-risk industry for exploitation. Being on a work visa may further exacerbate workers’ vulnerability in this sector by limiting workers’ options, including the ease of changing jobs. The rapid increase in the number of care workers on work visas from early 2022 onwards increases the scale of the monitoring challenge. While health does not have the same high-risk status as care, media reports have also identified cases of high exit fees for NHS nurses – although it is not clear how widespread this practice is.
If policymakers want to reduce reliance on overseas health workers, can they do it? In theory, it does. The government has more control over the health and care labour markets than most other sectors. Government bodies fund training places and set pay and conditions in the NHS. They also indirectly influence pay and conditions in social care, where private-sector organisations are commissioned by local authorities using public funding. In principle, therefore, it has levers to increase the pipeline of domestic workers. Pulling these levers, for example, by increasing the number of training places or making pay more attractive, has a cost. Policymakers thus face a trade-off between the ease and comparatively low cost of short-term reliance on overseas workers and the longer-term risks of shocks to international recruitment and challenges monitoring working conditions.
Finally, there are some key evidence gaps and limitations. Geographical coverage on the non-UK national or non-UK born workforce across the UK is uneven. England has more detailed data for NHS staff (through NHS Digital) and care workers (through Skills for Care). Coverage in Wales, Scotland and Northern Ireland is more limited, although GMC and NMC registration data provide useful data.
Given the importance of international recruitment in the current health and care workforce, more detailed data on the outcomes and retention of recent international recruits would greatly improve understanding of their role in the workforce. For example, Home Office statistics provide information on the ‘stay rates’ of work visa holders by nationality but not by occupation or industry. Data on movement between industries – for example, migrants’ propensity to move in and out of health jobs – could, in theory, be derived from HMRC records and would also help illuminate the factors affecting retention.
Appendices
Appendix Figure A
Appendix Figure B
Acknowledgements
Research for this project was produced with the support of the NHS Confederation and Trust for London. Thanks to Mark Dayan, Lucinda Rolewicz, William Palmer, and Chris Warhurst for comments on an earlier version of this briefing. Thanks to Hector Hurmuz-Sklias for creating the visualisations.
This paper was authored for ReWAGE. It represents the views of the authors based on the available research. It is not intended to represent the views of all ReWAGE members.
ReWAGE is an independent expert advisory group modelled on SAGE that is co-chaired by the Universities of Warwick and Leeds. It analyses the latest work and employment research to advise the government on addressing the challenges facing the UK’s productivity and prosperity, such as Covid-19, the cost-of-living crisis and labour shortages. For more information, visit https://warwick.ac.uk/fac/soc/ier/rewage/. ReWAGE is primarily funded by the Economic and Social Research Council.